45 yr old female patient with complaints of vomiting since 10 days and H/o renal stones
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 45 year old female patient came OPD with
Chief complaints: Nausea & Vomiting since 10 days .
HOPI: Pt was apparently asymtomatic 10 days ago and then developed nausea and vomiting.
Associated with decreases appetie and disturbed sleep.
She had 4-5 episodes per day in the last two days.
It occured few hours after consumption of food.
Contents :- food particles
DAILY ROUTINE :
The patient wakes around 6 am and does all her household chores,cook food, prepare her kids for school and goes to do her work in field.
She has her lunch by 1 pm and then takes an half an hour rest and then gets back to work.
She returns home by 6pm , freshen up and then prepare dinner.
She has her dinner with family by 8 pm then watches T.V. till 9:30 pm and then goes to sleep
EVENTS LEADING TO FIRST EPISODE OF VOMITING :
She woke up as per her daily routine and did all her household work went to work with her husband by afternoon after having her lunch she felt nauseous and had her first episode of vomiting.
Then 4 such episodes happen in quick succession even after consuming just water.
Then her husband got to the hospital.
PAST HISTORY : she is not a known case DM, HTN, TB
4 years ago she had complaints of burning micturition, fever and pedal edema for which she consulted a local doctor.
She was found to have right kindney stones with infection and simple right nephrectomy done in 2018.
Then she was adviced for a follow up every 6 months,which she did go for 2 yr years and then didnt due to personal reasons.

FAMILY HISTORY: No similar complaints in the family.
PERSONAL HISTORY:
Diet: mixed
Appetite: normal
Sleep: adeqaute
Bowel and bladder : regular
Addictions : none
GENERAL EXAMINATION :
Pt was conscious, coherent and cooperative.
She was well oriented time, place and person.


Cyanosis : none
Clubbing : none
Lymphadenopathy : none
Edema : none
VITALS
BP : 130/80 mm hg
PR : 82 bpm
RR : 16 cpm
TEMPERATURE : afebrile
SPO2 : 98%


SYSTEMIC EXAMINATION :
CVS : S1 & S2 heard and no murmurs noticed
Respiratory System : Bilateral air entry present and vesicular breath sounds heard.
Abdominal system : on inspection : normal.
on palpation : no tenderness seen in any quandrant.
on auscultation : bowel sounds heard.
CNS : no focal neurological defects seen.
INVESTIGATIONS :
USG - ABDOMEN : 4 Years ago


CBP :  CUE :
CUE : 
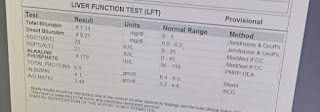
LFT :


ECG :
 ON 30/6/22:
ON 30/6/22:Now she has B/L pedal edema extending upto knees and facial puffiness too.




INVESTIGATIONS ORDERED :
HEAMOGRAM
BUN
RFT



On 4/7/22
Vitals
BP : 150/80 mm Hg
PR : 90 bpm
CVS : s1 and s2 heard
CNS : no focal neurogical defects
RS : BAE +
Investigations done
BUN



Feature 25th 30th 4th
Pedal edema absent present absent
extending
upto kness
Hb 13.7 6.9 6.7
(Normal) (decreased) (decreased)
Urea 113 101 126
S.creatinine 6.0 6.9 6.6
PROVISIONAL DIAGNOSIS :
AKI secondary to gastroenteritis.
TREATMENT :
27/6/22
Inj.PAN 40mg /IV /OD
Inj. METROGYL 50mg / IV /TID
Inj. ZOFER 4mg / IV
Tab. DOLO 650 mg
IVF NS @ 40 + 50 ml/hr
28/7/22 -4/7/22
T. LASIX 20mg / PO/BD
T. NODOSIS 500mg / PO/ BD
T. MVT /PO/OD
T. SHELCAL 500mg /PO/ OD
Cap. Bio-D3/PO/OD
T.NICARDIA 10mg /PO/BD

{kind=link}
{kind=link}
Comments
Post a Comment