This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
This is a case of a 75 year old lady who presented with weakness of right upper and lower limbs and slurring of speech since one day
HISTORY OF PRESENTING ILLNESS
The patient was apparently asymptomatic until 4 months ago and then she began experiencing bilateral knee pains right leg greater than the left leg. She went to the hospital and was given treatment
Events leading to the current presentation:
The patient woke up in the morning as usual and did her daily chores which comprise of sweeping the house and other activities and had lunch at 12 and then had an afternoon nap. When she woke up she was not able to get out of the bed and was not able to move her right upper and lower limb. She also experienced slurring of speech and there is also a change in voice.
Not associated with blurring/diminision of vision, dizziness, numbness of tongue
No c/o weakness of limbs,seizures,headache,sensory symptoms
No c/o burning micturition,cough,SOB,vomiting,loose stools
No H/o head trauma.
Daily Routine:
The patient’s attender remarked that the patient was a very active person and is an amicable person. She wakes up at 6 AM and sweeps the house after freshening up. She helps in minor chores around the house. She has lunch at 12 and sleeps for some time in the afternoon. After she wakes up she chats with the neighbours and has dinner at 7 and sleeps by 8 PM.
PAST HISTORY
The patient was diagnosed with hypertension 15 years back and is on medication since then
The patient also has frequent bloating and epigastric pain and uses medication
No history of diabetes, epilepsy, asthma, thyroid disorders
TREATMENT HISTORY
Etizolam
Rabeprazole sodium and levosulpride
Cinod-T
PERSONAL HISTORY
Diet: mixed
Appetite: normal
Sleep: unable to sleep, experiences sleep disturbances. Uses etizolam
GENERAL EXAMINATION
Patient is conscious coherent and cooperative. Well oriented to time place and person
Pallor absent
Icterus absent
Clubbing absent
Cyanosis absent
Lymphadenopathy absent
Edema absent
Vitals
BP 141/90
PR 75 BPM
Temp afebrile
RR 16
CNS EXAMINATION
HIGHER MENTAL FUNCTIONS:
Conscious, oriented to time place and person.
speech : slurred, unable to pronounce cha, ja, va(12th cranial nerve?)
Behavior : normal
Memory : Intact.
Intelligence : Normal
Lobar Functions : Normal.
No hallucinations or delusions.
CRANIAL NERVE EXAMINATION:
1st : Normal
2nd : visual acuity is normal
3rd,4th,6th : pupillary reflexes present.
EOM full range of motion present
gaze evoked Nystagmus present.
5th : sensory intact
motor intact
7th : angle of mouth deviated to left side. loss of nasolabial fold on right side
8th : No abnormality noted.
9th,10th : palatal movements present and equal.
11th,12th : normal.
MOTOR EXAMINATION: Right Left
UL LL UL LL
BULK Normal Normal Normal Normal
TONE hypotonia hypotonia normal normal
POWER 0/5 2/5 5/5 5/5
SUPERFICIAL REFLEXES:
CORNEAL present present
CONJUNCTIVAL present present
PLANTAR withdrawal withdrawal
DEEP TENDON REFLEXES:
BICEPS 3 2
TRICEPS 3 2
SUPINATOR 1 2
KNEE - -
ANKLE 3 1
SENSORY EXAMINATION:
SPINOTHALAMIC SENSATION:
Crude touch diminished on right upper limb
pain diminished on right upper limb
DORSAL COLUMN SENSATION:
Fine touch not able to perceive on right upper and lower limb
Proprioception normal
CORTICAL SENSATION:
Two point discrimination unable to discrimate on right upper and lower limb
Tactile localisation unable to do on right upper and lower limb
CEREBELLAR EXAMINATION:
Finger nose test unable to preform with right hand
Heel knee test unable to preform with right lower limv
Dysdiadochokinesia not able to preform with right hand
Nystagmus not seen
Titubation not present
SIGNS OF MENINGEAL IRRITATION: absent
GAIT:
unable to stand without support
unsteady with a tendency to fall
unable to perform tandem walking.
CVS S1 S2 heard, no murmurs
RS BAE, no added breath sounds
ABDOMEN soft and non tender
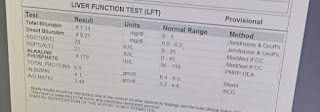
INVESTIGATIONS
PROVISIONAL DIAGNOSIS:
CVA with right hemiparesis secondary to acute infarct in left putamen









Comments
Post a Comment